
Dr. Anam Tariq presents chronic kidney disease (CKD.) In the part one she discusses the following topics:
Learning objectives of this video are the following:
1. Definition of Chronic Kidney Disease (CKD).
2. Stages of CKD.
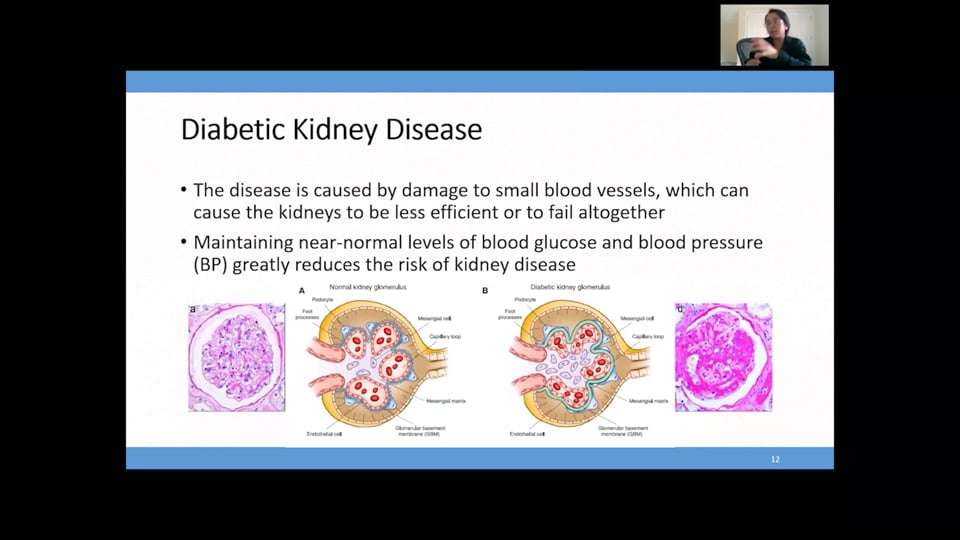
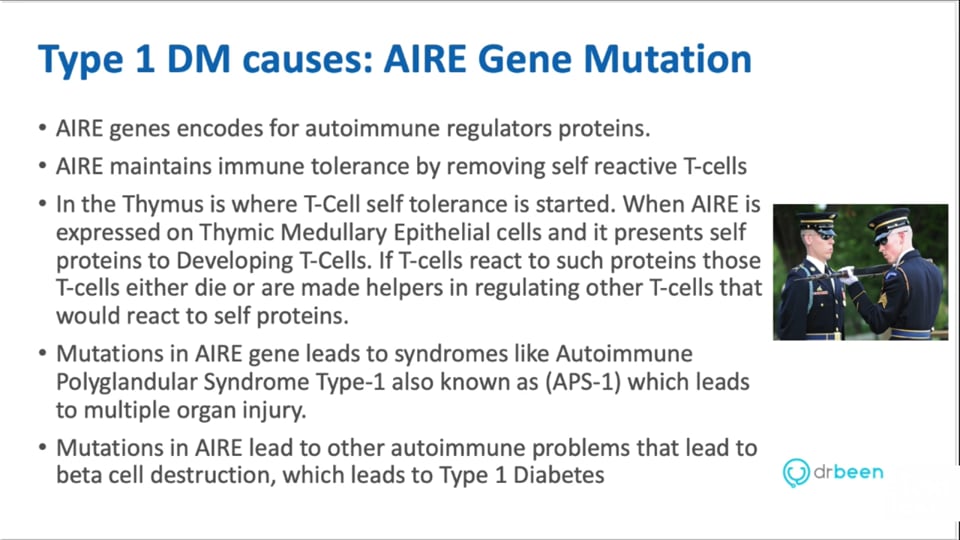
3. Causes
4. Albuminuria - Biomarker use & limitations
5. Albuminuria & cardiovascular Disease
6. Prognosis of CKD by GFR & albuminuria categories : KIDGO 2012
Presented by Dr. Anam Tariq
Following answers are created by ChatGPT. Occasionally the answer may be harmful, incorrect, false, misleading, incomplete, or limited in knowledge of world. Please contact your doctor for all healthcare decisions. Also, double check the answer provided by the AI below.
No credit card information needed.
 1.75 CME
1.75 CME
Amr Madkour, MD
Ahmed Zaafran, MD
 1.25 CME
1.25 CME
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Dr. Mobeen Syed
Dr. Anam Tariq
Dr. Anam Tariq

Dr. Anam Tariq
John Prietto
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.17 CME
0.17 CME
Dr. Mobeen Syed
 0.17 CME
0.17 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed

Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
All information contained in and produced by DrBeen corp is provided for educational purposes only. This information should not be used for the diagnosis or treatment of any health problem or disease.
THIS INFORMATION IS NOT INTENDED TO REPLACE CLINICAL JUDGMENT OR GUIDE INDIVIDUAL PATIENT CARE IN ANY MANNER.
Click here for notice and disclaimer.
Write A New Comment
2 Comments
ctrevascus@*.com
Dec 27 2020, 6:08 am
Thank you. I would love to know more about interpreting results in patients with CKD and heart failure. Particularly urea and urea creatinine ratio. When to diurese and when to look elsewhere for causes of oedema such as lymphoedema I find this perplexing and would love some insight.
srtupper@*.com
Nov 23 2020, 6:59 pm
This is the 1st Dr. Been video I've watched and I thought it was well-presented in terms I could grasp. I really liked some of the graphics used. Thank you! I'm looking forward to PartII.
Thanks,
Sarah